
Better know your local districts, Part 1: The Point Roberts Organizational Chart
In their joint statements at the March meeting, Hospital District Superintendent Elaine Komusi and Unity Care COO Shanon Hardie used some form of the word “partner” seven times when describing the relationship between the district and Unity Care. The Commissioners and Superintendent have also described the relationship as a "partnership" many times in the past. The district and Unity Care can be justifiably proud of their close working relationship. However, while they may believe that their “partnership” is their greatest strength, it is also their greatest weakness.
What’s wrong with a taxing district considering itself to be "partners" with their contractor?
For one thing, it makes the contractor a co-equal with the district and dilutes the district’s authority to manage the contractor. The district Commissioners’ fiduciary responsibility is to the Point Roberts taxpayers, not to their contractor. When Unity Care convinced the district to pay for their branding sign, the sign itself was a minor matter, but it signified larger and more pervasive issues of the district's governance and loyalty.
Businesses and public entities should operate based on laws and processes. A public taxing district has a bigger obligation to do so since they are managing taxpayer funds. However, the Hospital District has allowed personal trust to displace these processes and oversight. One way this was demonstrated was the fact that, until we brought it up last year, two Commissioners believed the Unity Care contract was multi-year (it's annual), and one didn't even know there was a contract with Unity Care despite being on the board for over nine years.
A partnership also conflates the district with the clinic and the contractor. Any challenge to the governance of the district is perceived as an attack on the clinic and on the contractor. Breaking down these boundaries has also allowed the contractor to get involved in local politics, which should be the sole realm of the district Commissioners. The contractor should be insulated from local politics; the district should make its decisions based solely on the community good and manage the contractor accordingly.
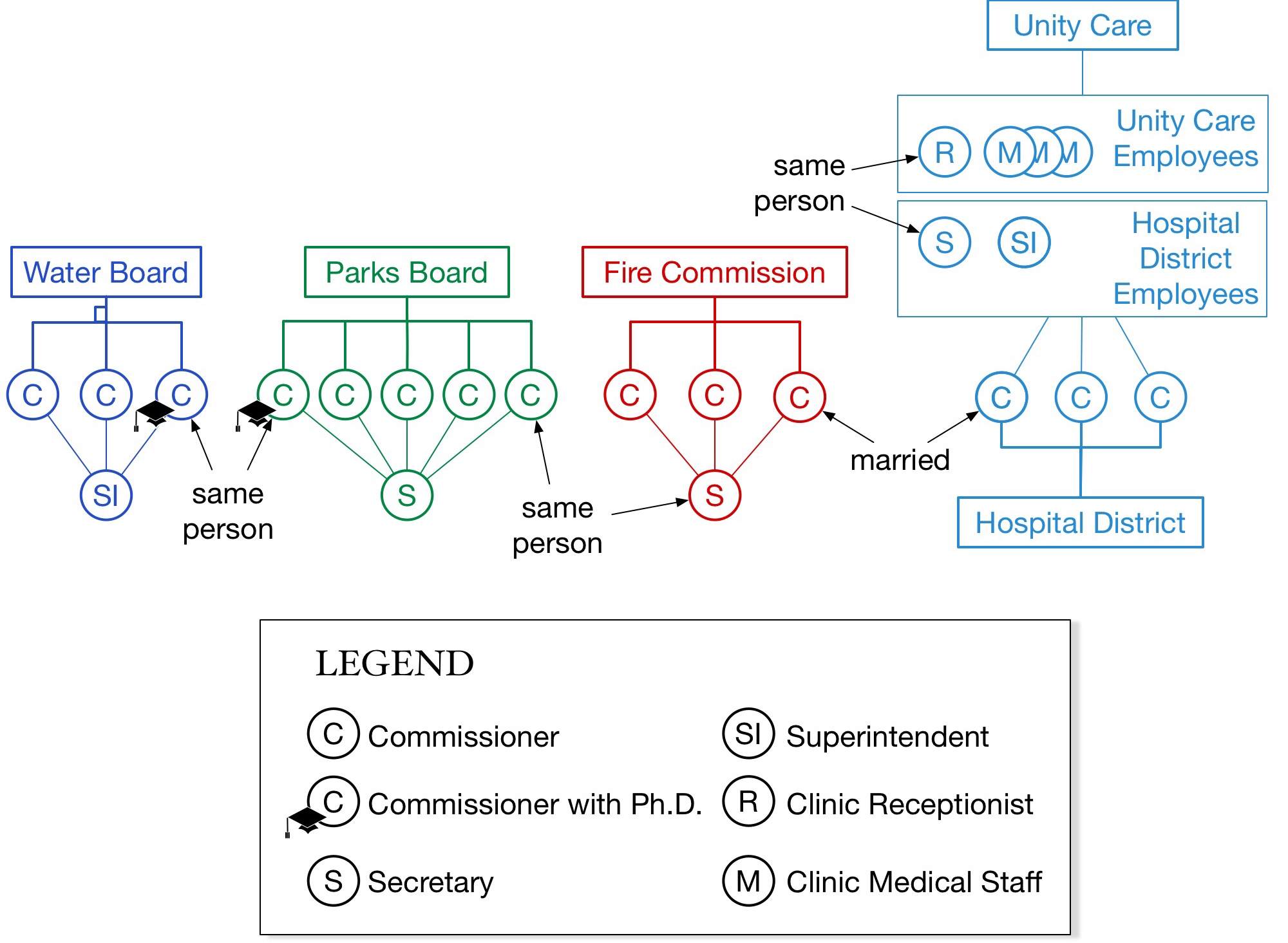
The most visible example of how these boundaries have been broken is the dual role of the clinic receptionist who also serves as the district recording secretary. She is employed by Unity Care in the first role and by the district (for 32 hours a month!) in the second. The practical result of this is that the district cannot conduct any business without a Unity Care employee being present. (This is the second conflict of interest from quiz question 1.)
In her statement in the March 1 meeting, Shanon Hardy said, “I want everybody to understand that this community has to decide if they want Unity Care here or not. We are happy to be here if they want us to be here.” The community survey that was just completed is the most objective measure of the community’s sentiment. It should be the basis for this decision.
Shanon Hardy also said, “I also want to say that it has been very difficult trying to think and respond to community feedback about, ok, so we need behavioral health services here, we need dental here, we need these things here. None of that is in our contract. Absolutely not one word. All that we’re obligated to do is medical. And we’ve tried very hard to respond to what the community here has asked of us, and tried to bring those services. And yet I’ve not seen from that small group not one ounce of credit for doing that. Not one ounce.” So here’s more than an ounce of credit. These are community needs, and Unity Care should be commended for going beyond the contract terms in trying to meet them. But a better way would be for the Hospital District to amend the contract to cover them.
Finally, the Commissioners and Superintendent have expressed concern in the past that Unity Care will leave and the clinic will close. Chairman Williams again raised this concern in the February meeting, citing the budget and dwindling reserve. Unity Care understands this: in the March meeting, Shanon Hardy said, "We’re not here because of us, we’re here because this was started ten years ago and if we leave, to my knowledge, there is no one who has shown any interest in being there. Which means the rest of the community will not have services." This gives Unity Care significant leverage over the district, and the "partnership" relationship enables that leverage.
If Unity Care does choose to leave, they will undoubtedly cite "dissent", but we believe it will be due to financial issues that were allowed to develop because management and governance were replaced by trust and "partnership".


New comic every Monday